Sunday, December 24, 2017
Wednesday, December 13, 2017

Bioterrorism; An emerging threat to World
Bioterrorism
A bioterrorism attack is
the deliberate release of viruses, bacteria, or other germs (agents) used to
cause illness or death in people, animals, or plants. These
agents are typically found in nature, but it is possible that they could be
changed to increase their ability to cause disease, make them resistant to
current medicines, or to increase their ability to be spread into the
environment. Biological agents can be spread through the air, through water, or
in food. Terrorists may use biological
agents because they can be extremely difficult to detect and do not cause
illness for several hours to several days. Some bioterrorism agents, like the smallpox
virus, can be spread from person to person and some, like anthrax, cannot.
History
— In
1984, in The Dalles, Oregon, U.S., a group of extremist followers of Bhagwan
Shree Rajneesh (also known as Osho) contaminated the salad in 10 different
salad bars with the pathogen of salmonellosis, Salmonella thyphimurium,
in order to disable the population. A
total of 751 people contracted the disease and several of them were
hospitalized. Although there were no fatalities, this terrorist act is
considered the largest bioterrorist attack in the history of the U.S. (Török et
al., 1997).
— In
the 1990s, the Japanese cult of Aum Shinrikyo tested different bioweapons,
including botulin toxin, anthrax, cholera, and Q fever.
— In
1993, during a humanitarian mission in Africa, it tried to obtain samples of
the Ebola virus.
— Between
1990 and 1995, the cult attempted to carry out several bioterrorist acts in
Tokyo using vaporized biological agents, including botulinum toxin and anthrax
spores. Fortunately, the attacks were unsuccessful (Olson, 1999).
— A
significant bioterrorist event occurred in the U.S. contextually to the
dramatic attacks to the World Trade Center in New York in September 2001. The
release of Bacillus anthracis spores through the U.S. postal system was
carried out with letters addressed to the press and to government officials. There
were 22 confirmed cases of anthrax contamination, consisting of 12 cutaneous
and 10 inhalational cases. The 12 cutaneous patients responded positively to
antibiotic treatment, while of the 10 inhalational cases, 4 were fatal
(McCarthy, 2001).
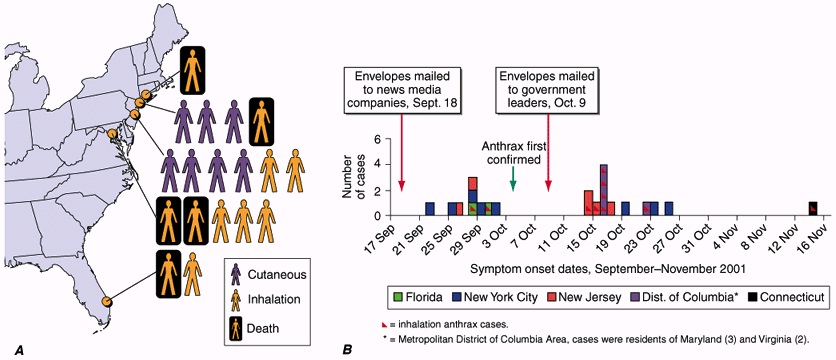
Figure showing Confirmed anthrax cases associated with bioterrorism: U.S.,
2001.
A. Geographic location and clinical manifestation of the 11 cases of confirmed inhalational and 7 cases of confirmed cutaneous anthrax.
B. Epidemic curve for the 18 confirmed cases of inhalational and cutaneous anthrax and 4 cases of suspected cutaneous anthrax.
A. Geographic location and clinical manifestation of the 11 cases of confirmed inhalational and 7 cases of confirmed cutaneous anthrax.
B. Epidemic curve for the 18 confirmed cases of inhalational and cutaneous anthrax and 4 cases of suspected cutaneous anthrax.
— In
2002, in Manchester, U.K., six terrorists were arrested for being found in
possession of ricin, and in 2004, traces of the same toxin were found at the
Dirksen Senate Office Building in Washington D.C. (Bhalla & Warheit, 2004).
— It
appears evident then that the use of biological agents has moved, in recent
times, to terrorist groups.
— This
creates very strong concerns that the use of bioweapons by terrorists can
create unexpected scenarios characterized by massive destructive potential
Bioterrorism agents’
important features of a perfect BW are:
- Highly
infectious and highly effective.
- Easily
produced with a long shelf life.
- Efficiently
dispersible.
- Readily
grown and produced in large quantities.
- Stable
on storage.
- Resistant
enough to environmental conditions.
- Resistant
to treatment
- High morbidity and mortality
- Potential for person-to-person spread
- Low infective dose and highly infectious by aerosol
- Lack of rapid diagnostic capability
- Lack of universally available effective vaccine
- Potential to cause anxiety
- Availability of pathogen and feasibility of
production
- Database of prior research and development
- Potential to be “weaponized”
Category of Bioterrorism
by Centers for Disease Control and Prevention (CDC):
The U.S. Centers for
Disease Control and Prevention (CDC) defines a bioterrorism attack as “the
deliberate release of viruses, bacteria or other germs (agents) used to cause
illness or death in people, animals, or plants” (CDC, 2013). It classifies biological agents into three
categories
Category A:
·
The U.S. public health system and primary
healthcare providers must be prepared to address various biological agents,
including pathogens that are rarely seen in the United States.
·
High-priority agents include organisms
that pose a risk to national security because they can be easily disseminated
or transmitted from person to person;
·
result in high mortality rates and have
the potential for major public health impact;
·
might cause public panic and social
disruption; and
·
require special action for public health
preparedness.
Groups
|
Diseases
|
Agents
|
A
|
Anthrax
|
Bacillus anthracis
|
Botulism
|
Clostridium botulinum toxin
|
|
Plague
|
Yersinia pestis
|
|
Smallpox
|
Variola major
|
|
Tularemia
|
Francisella tularensis
|
|
Viral hemorrhagic fevers
|
Filoviruses (e.g.
Ebola, Marburg) and Arenaviruses (e.g. Lassa, Machupo)
|
Category B:
— Second
highest priority agents include those that are moderately easy to disseminate;
— result
in moderate morbidity rates and low mortality rates; and
— require
specific enhancements of CDC's diagnostic capacity and enhanced disease
surveillance.
Groups
|
Diseases
|
Agents
|
B
|
Brucellosis
Epsilon toxin
|
Brucella spp.
Clostridium perfringens
|
Food safety threats
|
Salmonella spp.,
E.coli O157:H7, Shigella
|
|
Glanders
|
Burkholderia mallei
|
|
Melioidosis
|
Burkholderia pseudomallei
|
|
Psittacosis
|
Chlamydia psittaci
|
|
Q fever
|
Coxiella burnetii
|
|
Ricin toxin
|
Ricinus communis
|
|
Staphylococcal enterotoxin
B
|
Staphylococcus spp.
|
|
Typhus fever
|
Rickettsia prowazekii
|
|
Viral encephalitis
|
Alphaviruses (e.g.
Venezuelan equine encephalitis, Eastern equine encephalitis, Western equine
encephalitis
|
|
Water safety threats
|
Vibrio cholerae,
Cryptosporidium parvum
|
Category C:
— Third
highest priority agents include emerging pathogens that could be engineered for
mass dissemination in the future because of availability;
— ease
of production and dissemination; and
— potential
for high morbidity and mortality rates and major health impact.
|
Groups
|
Diseases
|
Agents
|
|
C
|
Emerging infectious diseases
|
Nipahvirus and
Hantavirus
|
Other classifications:
Generally, biological
agents (included those used as bioweapons) can be further classified according
to certain characteristics that define the hazard to health (NATO, 1996):
a.
Infectivity: The
aptitude of an agent to penetrate and multiply in the host.
b.
Pathogenicity: The
ability of the agent to cause a disease after penetrating into the body.
c.
Transmissibility: The
ability of the agent to be transmitted from an infected individual to a healthy
one
d.
Ability to neutralise: Its
means to have preventive tools and / or therapeutic purposes.
Transmissions:
Biological agents can be
transmitted through one or more ways.
The transmission modes are the following:
- Parenteral: Agents
that are transmitted through body fluids or blood.
- Airway (by droplets): Agents
that are emitted by infected people, which can then be inhaled by
surrounding people.
- Contact: Through
which the agents present on the surface of the infected organism can
infect another organism.
- Oral-faecal route: Through
objects, foods or other items contaminated with the faeces of infected
patients, or through sexual contact.
Impacts of Bioterrorism:
— Economic
impact of a bioterrorism attack could be devastating.
— Cost
$23 million to decontaminate a government building after 2001 anthrax attacks
in the US.
— Early
intervention can significantly decrease the costs resulting from a bioterrorist
attack.
— Still
expensive to provide prophylactic antibodies to a large number of individuals
— Reduction
in hospital admissions greatly outweighs initial costs
Warning signs:
— In
any location hit by a bioterrorism act the public health system will probably
be first to detect and respond.
— May
not be realistic to wait for confirmation of diagnosis.
— Delay
increases the potential for spread.
— Emergency
response may need to be activated on basis of patterns and timing of patient
presentation.
— Important
clues that can help alert hospitals to bioterrorist attack
— Every
health care professional should be suspicious of any unusual activity.
— It
will take many people in a variety of fields to control the impact of a
biological attack.
— Veterinarians
–many infectious diseases are zoonotic
— Scientists,
epidemiologists, doctors, and nurses will need to work together.
— Law
enforcement –reporting disease and controlling public reaction
— Bioterrorism
is a matter of national and international security.
— Require
the coordination of local, state, federal, and international agencies
Individual role
— It
is imperative that you understand your role.
— Prepare
ahead of time.
— Become
familiar with the location of important telephone numbers and resources.
— Then
you will be ready to assist at a moment’s notice.
— Your
day-to-day responsibilities may be much different during the response to a
bioterrorist attack.
— First
step is notifying the proper officials.
— Know
how to contact these agencies in advance.
— This
may save crucial minutes during a time of chaos.
Bacteria in Photos