MONKEYPOX

Classification:
Group: Group I (double-stranded DNA virus)
Family: Poxviridae
Subfamily: Chordopoxvirinae
Genus: Orthopoxvirus
Species: More than ten species including smallpox, monkeypox, cowpox, horsepox,
etc.
Virion Structure:
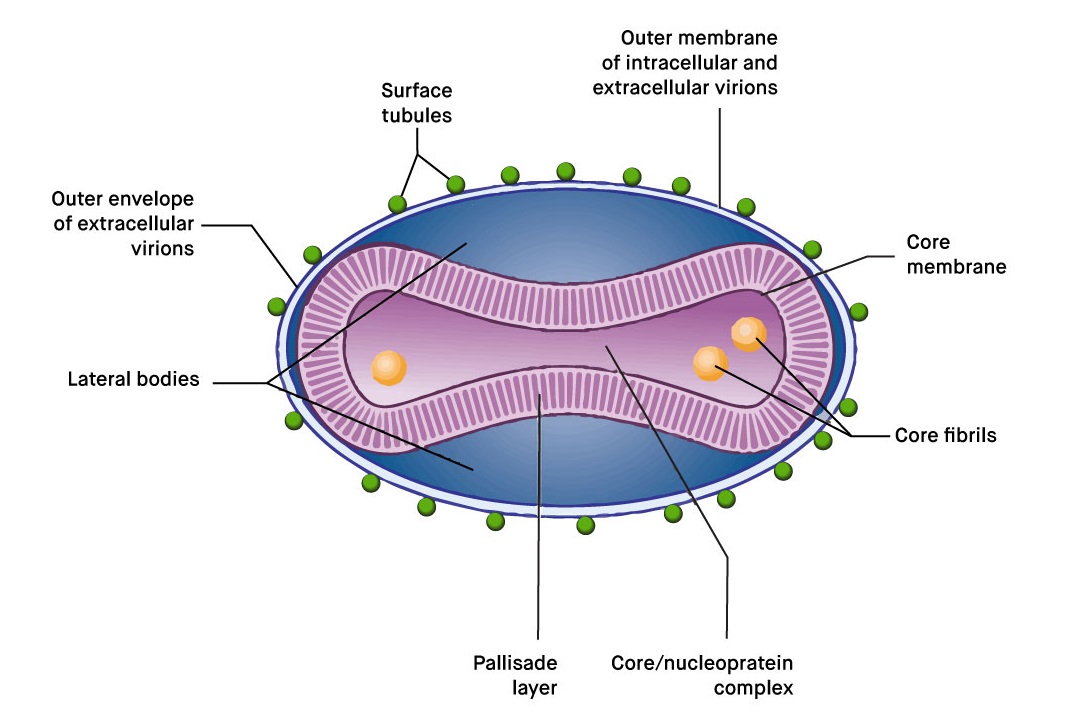
Virion: Complex structure,
oval or brick-shaped, 400 nm in length x 230 nm in diameter; external surface
shows ridges; contains the core and lateral bodies
Composition: DNA (3%), protein
(90%), lipid (5%)
Genome: Double-stranded DNA,
linear; size 130–375 kbp; has terminal loops; has low G + C content (30–40%)
except for Parapoxvirus (63%)
Proteins: Virions contain more
than 100 polypeptides; many enzymes are present in the core, including the transcriptional system
Envelope: Virion assembly
involves the formation of multiple membranes
Replication: Cytoplasmic
factories
Outstanding characteristics:
Largest and most
complex viruses; very resistant to inactivation
Virus-encoded
proteins help evade the host immune defense system
Member of same
genus with Smallpox which was the first viral disease eradicated from the
world and also with cowpox and horsepox
Outbreak:
On 14 May 2022, a familial cluster of two cases of monkeypox
was reported in the United Kingdom (UK) by the UK Health Security Agency
(UKHSA). These cases have no relation to a travel-related case from Nigeria
that was previously reported on 7 May 2022 in the UK. Since the UKHSA reporting
of cases, several other European countries have reported cases of monkeypox.
As of 19 May 2022, 38 cases have been confirmed
worldwide. Of these, 26 cases have been confirmed in the following EU/EEA
countries: Belgium (2), France (1), Italy (1), Portugal (14), Spain (7), and
Sweden (1). In the UK, nine cases have been confirmed. In North America, three
cases have been confirmed in Canada (2), and the US (1). The majority of cases
have been in young men, many self-identifying as men who have sex with men
(MSM), and none with recent travel history to areas where the disease is
endemic. No deaths have been reported so far, and only two cases have been
admitted to hospital for reasons other than isolation.
Epidemiological update:
Since the disease was first detected on 7 May 2022 in the
United Kingdom, a total of nine cases have been confirmed in the United
Kingdom. Eight of the nine cases have no travel history and have no relation to
the travel related case confirmed on 7 May.
Since the UKHSA reporting of cases, in the EU/EEA, a
further 26 cases have been confirmed since 18 May in Belgium (2), France (1),
Italy (1), Portugal (14), Spain (7), and Sweden (1). Portugal has reported
another 20 suspected cases, and Spain has reported another 23 suspected cases
which are awaiting laboratory confirmation.
In total, since 14 May, there have been 37 confirmed,
non-travel related cases of monkeypox worldwide, with 26 in EU/EEA countries.
The majority of cases are in young men, self-identifying as MSM. There have
been no deaths, and two hospitalizations for reasons other than isolation were
reported worldwide. Health authorities across counties have stated that further
cases are expected. Below is a breakdown of the reporting countries:
- two cases have been confirmed in
Belgium
- one case has been confirmed in
France
- one case has been confirmed in
Italy, with 2 suspected cases identified
- 14 cases have been confirmed in
Portugal, with an additional 20 suspected cases identified
all in the Lisbon & Tagus River region
- seven cases have been confirmed
in Spain, with 23 suspect cases identified
- one case has been confirmed in
Sweden
- nine cases have been confirmed
in the United Kingdom
- two cases have been confirmed in
Canada, with an additional 17 suspected cases identified
- one confirmed and one probable case in the US
- one confirmed case in Australia
The majority of cases have been in young men, many
self-identifying as men who have sex with men (MSM), and none with recent
travel history to areas where the disease is endemic. Most cases presented with
lesions on the genitalia or peri-genital area, indicating that transmission
likely occurs during close physical contact during sexual activities. This is
the first time that chains of transmission are reported in Europe without known
epidemiological links to West or Central Africa, where this disease is endemic.
These are also the first cases worldwide reported among MSM.
Disease background and
transmission:
This is the first time that chains of transmission are
reported in Europe without known epidemiological links to West or Central
Africa. These are also the first cases worldwide reported among MSM. The monkeypox
virus is considered to have moderate transmissibility among humans and can be
transmitted through droplets and/or contact with infected lesions. Transmission
between sexual partners, due to intimate contact during sex with infectious
skin lesions seems the likely mode of transmission among MSM.
Given the unusually high frequency of human-to-human
transmission observed in this event, and the probable community transmission
without history of traveling to endemic areas, the likelihood of further spread
of the virus through close contact, for example during sexual activities, is
considered to be high. The likelihood of transmission between individuals
without close contact is considered to be low.
The clinical manifestation of monkeypox is usually mild. The West African
clade, which has so far been detected in the cases reported in Europe, has been
observed to have a case fatality rate of about 3.3% in
Nigeria. Mortality is higher among children and young adults, and
immunocompromised individuals are especially at risk of severe disease. Most
people recover within weeks.
Immediate
recommendations:
Public health institutions/authorities and
community-based organizations should take steps to raise awareness on the
potential spread of monkeypox in the community, especially among men who have
sex with other men that engage in casual sex, or who have multiple sexual
partners. Individuals engaging in casual sex or who have multiple sexual
partners who are not MSM should also be vigilant. Any persons presenting with
symptoms indicative of monkeypox should seek specialist care and should abstain
from sexual activities or any other type of activities involving close contact
until monkeypox is either excluded or the infection is resolved.
Suspected cases should be isolated and tested and notified promptly. Back-wards
and forwards contact tracing should be initiated for positive cases, and
exposed mammalian pets should be quarantined. If smallpox vaccines are
available in the country, vaccination of high-risk close contacts should be
considered after a risk-benefit assessment. For severe cases, treatment with a
registered antiviral can be considered, if available in the country.
ECDC actions :
ECDC will continue to
monitor this event through epidemic intelligence activities and report relevant
news on an ad-hoc basis. ECDC published a news item on 19 May, with initial
recommendations. An epidemiological update will be posted on 20 May. Multi-lateral
meetings between affected countries, WHO IHR and ECDC have taken place to share
information and coordinate response. A process in EpiPulse has been created to
allow countries to share information with one another, WHO, and ECDC. The
production of a Rapid Risk Assessment has been launched with prospective
publication on Monday 23 May.
Source:https://www.ecdc.europa.eu/en/news-events/epidemiological-update-monkeypox-outbreak