Giardiasis is a water borne
parasitic infection caused by protozoa, Giardia duodenalis. It is the third
most common cause of diarrhea after Rota virus and Cryptosporidium app. The
chronicity of diarrhea caused by G. duodenalis is more common than of
cryptosporidium spp even in the immunocompetent hosts. However, most of cases
of giardiasis is asymptomatic (around 69%). They are widely distributed worldwide
and more prevalent in the countries with poor sanitation and bad food hygiene
practices especially in the developing and under developed countries.
Life cycle:
There are two distinct forms of
the protozoa, trophozoites and cysts form.
1. Trophozoites
are motile form and show the falling leaf like motility. They possess four
pairs of flagella measuring about 12-15 and 5-15 micrometer in diameter. It
contains two nuclei and with the help of flagella it attaches to intestinal
mucosa by sucking discs. They multiply by longitudincal binary fission. No
Sexual reproduction has been reported yet in the giardia.
2. Cyst
form of Giardia is infective form with thick wall. The cyst form contains four
nuclei and size ranges from 8-14 micrometer. A cyst divides to give two
trophozoites.
Human get infected with ingested
of contaminated water with infective cyst forms. Once this cyst forms crosses
the acid barrier of stomach, they start excyst in small intestine to form two
trophozoites. They favor alkaline pH of duodenum and jejunum. The attach to the
small intestine microvilli via the sucking discs and move freely to the lumen
actually to the soft mucosa and submucosa. Unlike the cyrtosporidium they don’t
invade the tissue and just attach on microvilli and damage it causing
malabsorption and diarrhea.
Sometimes trophozoites can also
be seen in the stool but they can’t tolerate the extreme environmental
condition outside, however cysts can resist and hence use for diagnosis.
Trophozoites multiply by
longitudinal binary fission, remaining in the lumen of the proximal small bowel
where they can be free or attached to the mucosa by a ventral sucking disk.
Encystation occurs as the parasites transit toward the colon. The cyst is the
stage found most commonly in non-diarrheal feces. Because the cysts are
infectious when passed in the stool or shortly afterward, person-to-person
transmission is possible. While animals are infected with Giardia,
their importance as a reservoir is unclear.

Classification:
Altogether there are 9
assemblages of Giardia spp. named as A, B,C, D, E, F, G and H. The assemblages A and B are only found to
infect the humans, medically important species.
Assemblage A. Zoonotic and
anthroponotic transmission (primates, dogs, cats) and reported from diarrheal
stool samples of India, Spain and Turkey.
Assemblage B. It is also
transmitted by zoonotic and anthroponotic routes but only reported in Malaysia,
Netherland and Ethiopia.
Pathogenesis:
The major virulence’s factors of
Giardia spp are flagella and antigenic variations, variant-specific surface proteins (VSPs) among
the species. A dense coat of
VSPs covers the surface of Giardia trophozoites, and a single VSP is
normally dominating in a population of parasites, which is used by the protozoa
to escape the immune response of the host. The
antigenic variation also induces immune response of host and the damage is due
to host inflammatory response to giardia. The protozoa can also damage the
microvilli and lead to malabsorption.
The mechanism of pathogenesis for
Giardia is non invasive one unlike that of Crytosporidium spp. The protozoa
don’t penetrate the cells and their pathogenesis is not clearly understood.
Even 10 Giardia cysts can cause the infection to human.
After excystation, the motile
trophozoites are released into the small intestine. The trophozoites then
adhere to the epithelial cells via a specialize ventral suck device. The
protozoa and host cells attachment target specific signaling networks including
those of caspases. The caspases then activate the apoptosis mechanism leads to
death/loss of intercellular junctions. The reduced expression and relocation of
tight junctions such as Zo1, caudin-1, F-actin and alpha actinin result in
increased intestinal permeability and decreased transepithelial resistance. The
disruption also leads to cytoskeleton rearrangement and barrier dysfunction.
These mechanisms contribute to pathophysiological features such as paracellular
leakages-electrolyte secretion, malabsorption and finally to exudative
diarrhea. The tight junction alterations are associated to secretory diarrhea
due to an increase in chloride ion concentration and loss of absorptive
functions. The pathological observations on symptomatic has characteristic
features of villous shortening, microvilli atrophy and increase cell death and
destruction of the epithelial barriers. Consequently, enhanced fluid secretions
from the crypts cells is observed.

Clinical manifestations:
Commonly the clinical symptoms
manifest in 7-10 days and last for 1-3 weeks.
Most of symptomatic giardiasis have common symptoms like severe
diarrhea, abdominal cramps, bloating, flatulence, nausea and vomiting.
The chronic giardiasis in
immunocompromised individuals may have increases gas, dehydration, burping,
loose stools and slowed growth which may last for 2 months to years.
In both of the cases, weight loss
and dehydration are frequent.
Immune response by the host
Infection with Giardia is not
often accompanied by inflammation. The protozoa is poor cytokine inducer.
Higher prevalence of symptomatic Giardiasis is observed in infants and
self-limiting diarrhea is common in toddlers to endemic areas. Rarely
symptomatic infection occurs after pre-exposure. This shows the role of sIgA
antibody to prevent the infections. The neutralizing antibodies are the
protective immune response for Giardiasis. However, severe giardiasis mostly
occurs in underweight children with pre-existing malnutrition.
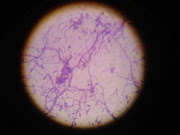
Laboratory Diagnosis
·
Light Microscopy: Iodine/Giemsa
·
Immunochromatography
·
Flow cytometry / ELISA
·
Molecular tools convention and real time PCR
Prevention
·
Good hygiene practice
·
Safe drinking water
·
Hand washing
·
Safe travelling