Asuma Gurung1 ߙ, Samjhana Gurung1 ߙ, Umesh Kaji Manandhar1, Raina Chaudhary2, Anand Kumar Mandal3 Avinash Chaudhary1, Dinesh Dhakal1, Anup Muni Bajracharya4, Upendra Thapa Shrestha5 *
1
Department
of Microbiology, Sainik Awasiya Mahavidhyalaya, Bhaktpur, Nepal
2
Shree Birendra Hospital Chhauni,
Kathmandu, Nepal
3 Department
of Pathology, Bhaktapur Hospital, Bhaktapur, Nepal
4
Balkumari
College, Chitwan, Nepal
5
Central
Department of Microbiology, Tribhuvan University, Kathmandu, Nepal
† These
authors contributed equally.
*Corresponding
author: Upendra Thapa Shrestha, Assistant
Professor, Central Department of Microbiology, Tribhuvan University, Kathmandu,
Nepal, E-mail: upendra.thapashrestha@cdmi.tu.edu.np
ABSTRACT
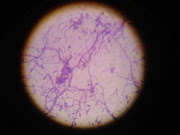
Objectives: To evaluate the antibiotic resistance pattern of Pseudomonas aeruginosa isolated from
clinical specimen and to detect Metallo beta lactamase producers as well as to accesses
their biofilm forming capacity by both qualitative and quantitative analysis.
Methods: The study was conducted in Shree Birendra Hospital, Chhauni,
from June to August 2025. The total of 6444 specimens was cultured and isolates
of P. aeruginosa were subjected to antibiotic susceptibility tests. Metallo
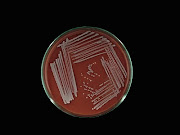
beta lactamase producers were identified by modified Hodge and EDTA synergy
tests. Biofilm was detected by the Congo Red Agar and Microtiter Plate Assay
method.
Results: Out of 671 positive
isolates (15.05%) from pus, urine and wound, 101 isolates of P. aeruginosa
were obtained. The highest rate of distribution was observed in in-patients as
well as in the age group of 61-70 years. Among the isolates, high resistance
was observed against Aztreonam (65.59%) whereas isolates were most sensitive against
Tobramycin (76%). 37 were found to produce Metallo beta lactamase enzyme and
almost 46% were MDR. The biofilm isolates
accounted for 34 by CRA but MPA detected 100 biofilm producers. The biofilm
producers showed high resistance against Aztreonam (59.41%) and Levofloxacin (56.44%).
Furthermore, the MBLS were the most resistant against Levofloxacin
(28.7%) followed by Aztreonam (27.7%), Cefepime (27.7%), Ceftazidime (25.7%),
Imipenem (25.7%) and Meropenem (25.7%). Out of all the isolates, 36
biofilm isolates were highlighted to produce MBL enzyme as well.
Conclusion: Pseudomonas aeruginosa was most frequent in sputum and pus samples from inpatients and older patients, with rising resistance to monobactams, fourth-generation cephalosporins, and fluoroquinolones. High rates of MBL production and biofilm formation contributed to marked β-lactam resistance, emphasizing the need for alternative therapeutic strategies.