May this new year 2023 bring all good innovations in science for human welfare!!

The importance of Epidemiology and Public Health is unavoidable in control of any infectious diseases.








Dengue is endemic in Nepal. The country is experiencing a surge
in cases that started from the week commencing 8 August to 26 August. Between
January to 28 September 2022, a total of 28 109 confirmed and suspected dengue
cases and 38 confirmed deaths due to dengue have been recorded, affecting all
seven provinces. The causative serotype(s) is unknown. This represents the
largest dengue outbreak in Nepal with regard to the cumulative number of cases
reported nationwide per year.
Description
of the outbreak
Between January and 28 September 2022, a total of 28 109
suspected and confirmed cases of dengue fever including 38 confirmed deaths
(overall CFR 0.13%) have been reported from all seven provinces of Nepal,
affecting all 77 districts in Nepal (Figure 1). Bagmati province which is the
second-most populous province has reported the highest number of cases (78.2%)
and deaths (68.4%).
According to the Epidemiology and Disease Control Division
(EDCD) of the Ministry of Health and Population, the highest number of new
cases in 2022 have been reported in the districts of Kathmandu (n=9528; 33.8%),
Lalitpur (n=6548; 23.2%), and Makwanpur (n=2776, 9.8%).
Data on demographics was available for 23% of cases (n= 6734) of
which 76% (5175/6734) were aged 15-59 years old, and 54% were males (n=3637).
As of 28 September, 38 deaths have been verified, of which males and cases aged
15 – 59 years old each accounted for 55% (n=21) of reported deaths. Cases aged
over 60 years old accounted for 39% (n=15) of reported deaths.
Dengue
cases have increased since July coinciding with the rainy season with majority
of the cases reported during September (83.6%; n=23 514).

Figure 1. Number of Dengue cases reported from
districts of Nepal from 1 January- 28 September 2022.

Figure 2. Number of dengue cases reported by
months in Nepal from 1 January to 28 September 2022
Source: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON412#:~:text=Dengue%20is%20endemic%20in%20Nepal,recorded%2C%20affecting%20all%20seven%20provinces.
If you know you have dengue, avoid getting further mosquito bites during the first week of illness. Virus may be circulating in the blood during this time, and therefore you may transmit the virus to new uninfected mosquitoes, who may in turn infect other people.
The proximity of mosquito vector breeding sites to human
habitation is a significant risk factor for dengue. At present, the main
method to control or prevent the transmission of dengue virus is to combat the
mosquito vectors. This is achieved through:
In addition, there is ongoing research amongst many
groups of international collaborators in search of novel tools and innovative
strategies that will contribute in global efforts to interrupt transmission of
dengue. The integration of vector management approaches is encouraged by WHO to
achieve sustainable, effective locally adapted vector control interventions.
Source: https://www.who.int/nepal/news/feature-stories/detail/continuing-the-fight-against-dengue


Antibiogram and Biofilm Development among Klebsiella pneumoniae from Clinical Isolates
Subash Paudel1, Laxmi Parajuli1, Prashanna
Adhikari1, Sanjay Singh K.C.2, Upendra Thapa Shrestha3, Pradeep Kumar Shah1*
1Department
of Microbiology, Tri-Chandra Multiple Campus, Kathmandu, Nepal
2Department
of Microbiology, SahidGangalal National Heart Center, Kathmandu, Nepal
3Central
Department of Microbiology, Kathmandu, Nepal
*Corresponding author: Pradeep Kumar
Shah; Department of Microbiology, Tri-Chandra Multiple Campus, Tribhuvan
University, Kathmandu, Nepal. Email: pkshah210@gmail.com
ABSTRACT
Objectives: This study was aimed to evaluate antibiotic
resistance pattern and biofilm formation in K. pneumoniae strains
isolated from different clinical specimens and to study on association of drug resistance
pattern with biofilm formation.
Methods: A total of 944 clinical samples from patients attending Sahid
Gangalal National Heart Center were processed from September 2019 to March 2020
to identify possible bacterial pathogens following standard microbiological
procedures. K. pneumonaie isolates were further subjected to antibiotic
susceptibility testing using modified Kirby Bauer disc diffusion technique.
Biofilm formation was evaluated by tissue culture plate technique.
Results: Of the total 944 samples, 146 (15.47%) samples showed bacterial
growth, among which 35 (23.97%) were K. pneumoniae. Out of 35 K.
pneumoniae isolates, 16 (45.71%) were multidrug-resistant and 15 (42.86%)
were extensively drug-resistant. Twenty-one (60%) K. pneumoniae feebly
produced biofilm. Significant association was observed between biofilm
production and exhibition of multidrug resistance (p < 0.05).
Conclusion: Prevalence of antibiotics resistant K.
pneumoniae in hospital setting is high and alarming. Significant association
between drug resistance pattern and biofilm production implicates need of an
immediate response to limit growth and spread of drug resistant microbes in
clinical settings.
Keywords: Kleibsella pneumoniae, multidrug resistance, biofilm,
antibiotic susceptibility test, Nepal
Citation: Paudel et al. Antibiogram
and Biofilm Development among Klebsiella pneumoniae from Clinical
Isolates. 2021, TUJM 8(1): 83-92. DOI: https://doi.org/10.3126/tujm.v8i1.41198
FULLTEXT: Download


Multidrug-resistant bacteria with ESBL genes: A growing threat among people living with HIV/AIDS in Nepal
Riju Maharjan1, Anup Bastola2, Nabaraj Adhikari1,
Komal Raj Rijal1, Megha Raj Banjara1, Prakash Ghimire1
Upendra Thapa Shrestha1*
1 Central Department of Microbiology, Tribhuvan
University, Kirtipur, Kathmandu, Nepal
*Corresponding author: Upendra Thapa Shrestha, Central
Department of Microbiology, Tribhuvan University, Kathmandu, Nepal, Email: upendrats@gmail.com / upendra.thapashrestha@cdmi.tu.edu.np
ABSTRACT
Background:
Bacterial opportunistic infections are common in people living with HIV/AIDS
(PLHA). Besides HIV-TB co-infection, lower respiratory tract infections (LRTIs)
due to multidrug-resistant (MDR) bacteria cause significant morbidity and
mortality among PLHA. This study identified bacterial co-infection of the lower
respiratory tract and detected plasmid-mediated blaTEM and blaCTX-M
genes among Extended-Spectrum b-Lactamase
(ESBL) producing isolates from sputum samples in PLHA.
Methods:
A total of 263 PLHA with LRTIs were enrolled in this study, out of which, 50
were smokers, 70 had previous pulmonary tuberculosis, and 21 had CD4 count
<200 cells/µl. Sputum samples collected from PLHA were processed with
standard microbiological methods to identify the possible bacterial pathogens.
The identified bacterial isolates were assessed for antibiotic susceptibility pattern
using modified Kirby Bauer disk diffusion method following Clinical Laboratory
Standard Institute (CLSI) guidelines. In addition, plasmid DNA was extracted
from MDR and ESBL producers for screening of ESBL genes; blaCTX-M and blaTEM
by conventional PCR method using specific primers.
Results:
Of 263 sputum samples, 67 (25.48%) showed bacterial growth. Among different
bacterial pathogens, Klebsiella
pneumoniae, (17; 25.37%) was
the most predominant, followed by Haemophillus influenzae, (14; 20.90%) and Escherichia
coli, (12; 17.91%). A higher infection rate (4/8; 50%) was observed among
people aged 61 -70 years, whereas no infection was observed below 20 years.
About 30.0% (15/50) of smokers, 32.86% (23/70) cases with previous pulmonary
tuberculosis, and 52.38% (11/21) with CD4 count <200 cells/µl had bacterial LRTIs.
Among 53 bacterial isolates excluding H. influenzae, 28 isolates were MDR
and 23 were ESBL producers. All ESBL producers were sensitive to colistin and polymyxin
B. Among ESBL producers, 47.83% (11/23) possessed blaCTX-M, 8.6% (2/23) were positive for blaTEM gene, and 43.48% (10/23)
possessed both ESBL genes.
Conclusion:
The increasing rate of MDR bacterial infections, mainly ESBL producers of LRTIs
causes difficulty in disease management, leading to high morbidity and
mortality of PLHA. Hence, it is crucial to know the antibiogram pattern of the
isolates to recommend effective antimicrobial therapy to treat LRTIs in PLHA.
Keywords: PLHA, Lower respiratory tract infection, ESBL, blaCTX-M, blaTEM
MONKEYPOX

Classification:
Group: Group I (double-stranded DNA virus)
Family: Poxviridae
Subfamily: Chordopoxvirinae
Genus: Orthopoxvirus
Species: More than ten species including smallpox, monkeypox, cowpox, horsepox,
Virion Structure:
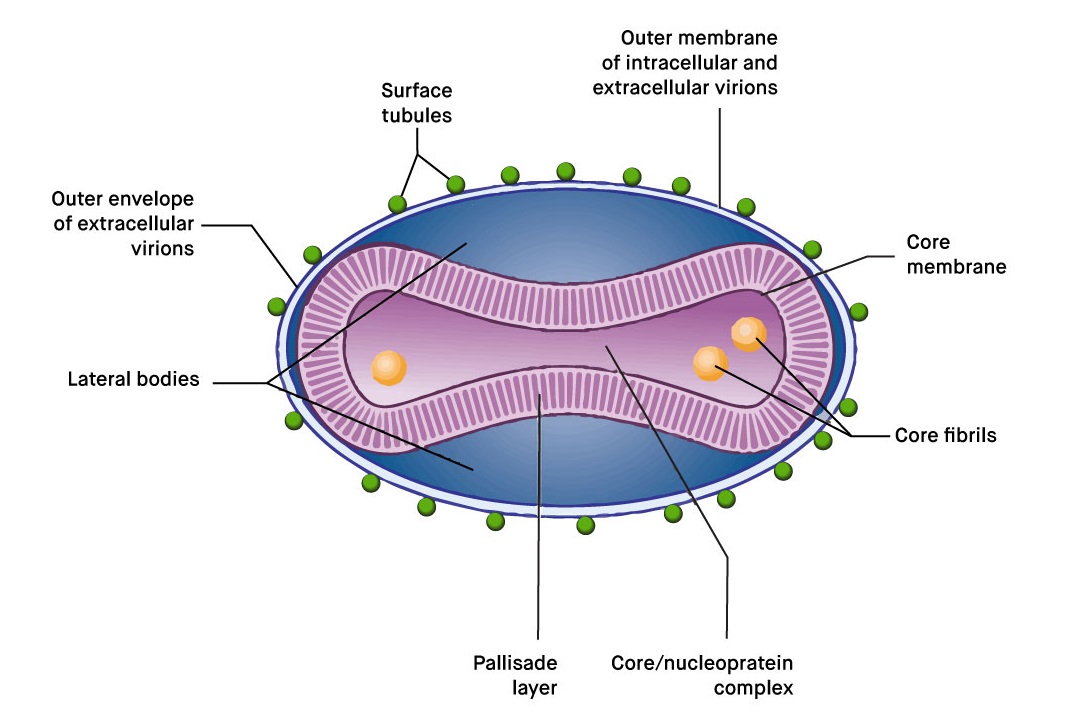
Virion: Complex structure,
oval or brick-shaped, 400 nm in length x 230 nm in diameter; external surface
shows ridges; contains the core and lateral bodies
Composition: DNA (3%), protein
(90%), lipid (5%)
Genome: Double-stranded DNA,
linear; size 130–375 kbp; has terminal loops; has low G + C content (30–40%)
except for Parapoxvirus (63%)
Proteins: Virions contain more
than 100 polypeptides; many enzymes are present in the core, including the transcriptional system
Envelope: Virion assembly
involves the formation of multiple membranes
Replication: Cytoplasmic
factories
Outstanding characteristics:
Largest and most
complex viruses; very resistant to inactivation
Virus-encoded
proteins help evade the host immune defense system
Member of same
genus with Smallpox which was the first viral disease eradicated from the
world and also with cowpox and horsepox
Outbreak:
On 14 May 2022, a familial cluster of two cases of monkeypox
was reported in the United Kingdom (UK) by the UK Health Security Agency
(UKHSA). These cases have no relation to a travel-related case from Nigeria
that was previously reported on 7 May 2022 in the UK. Since the UKHSA reporting
of cases, several other European countries have reported cases of monkeypox.
As of 19 May 2022, 38 cases have been confirmed
worldwide. Of these, 26 cases have been confirmed in the following EU/EEA
countries: Belgium (2), France (1), Italy (1), Portugal (14), Spain (7), and
Sweden (1). In the UK, nine cases have been confirmed. In North America, three
cases have been confirmed in Canada (2), and the US (1). The majority of cases
have been in young men, many self-identifying as men who have sex with men
(MSM), and none with recent travel history to areas where the disease is
endemic. No deaths have been reported so far, and only two cases have been
admitted to hospital for reasons other than isolation.
Epidemiological update:
Since the disease was first detected on 7 May 2022 in the
United Kingdom, a total of nine cases have been confirmed in the United
Kingdom. Eight of the nine cases have no travel history and have no relation to
the travel related case confirmed on 7 May.
Since the UKHSA reporting of cases, in the EU/EEA, a
further 26 cases have been confirmed since 18 May in Belgium (2), France (1),
Italy (1), Portugal (14), Spain (7), and Sweden (1). Portugal has reported
another 20 suspected cases, and Spain has reported another 23 suspected cases
which are awaiting laboratory confirmation.
In total, since 14 May, there have been 37 confirmed,
non-travel related cases of monkeypox worldwide, with 26 in EU/EEA countries.
The majority of cases are in young men, self-identifying as MSM. There have
been no deaths, and two hospitalizations for reasons other than isolation were
reported worldwide. Health authorities across counties have stated that further
cases are expected. Below is a breakdown of the reporting countries:
The majority of cases have been in young men, many
self-identifying as men who have sex with men (MSM), and none with recent
travel history to areas where the disease is endemic. Most cases presented with
lesions on the genitalia or peri-genital area, indicating that transmission
likely occurs during close physical contact during sexual activities. This is
the first time that chains of transmission are reported in Europe without known
epidemiological links to West or Central Africa, where this disease is endemic.
These are also the first cases worldwide reported among MSM.
Disease background and
transmission:
This is the first time that chains of transmission are
reported in Europe without known epidemiological links to West or Central
Africa. These are also the first cases worldwide reported among MSM. The monkeypox
virus is considered to have moderate transmissibility among humans and can be
transmitted through droplets and/or contact with infected lesions. Transmission
between sexual partners, due to intimate contact during sex with infectious
skin lesions seems the likely mode of transmission among MSM.
Given the unusually high frequency of human-to-human
transmission observed in this event, and the probable community transmission
without history of traveling to endemic areas, the likelihood of further spread
of the virus through close contact, for example during sexual activities, is
considered to be high. The likelihood of transmission between individuals
without close contact is considered to be low.
The clinical manifestation of monkeypox is usually mild. The West African
clade, which has so far been detected in the cases reported in Europe, has been
observed to have a case fatality rate of about 3.3% in
Nigeria. Mortality is higher among children and young adults, and
immunocompromised individuals are especially at risk of severe disease. Most
people recover within weeks.
Immediate
recommendations:
Public health institutions/authorities and
community-based organizations should take steps to raise awareness on the
potential spread of monkeypox in the community, especially among men who have
sex with other men that engage in casual sex, or who have multiple sexual
partners. Individuals engaging in casual sex or who have multiple sexual
partners who are not MSM should also be vigilant. Any persons presenting with
symptoms indicative of monkeypox should seek specialist care and should abstain
from sexual activities or any other type of activities involving close contact
until monkeypox is either excluded or the infection is resolved.
Suspected cases should be isolated and tested and notified promptly. Back-wards
and forwards contact tracing should be initiated for positive cases, and
exposed mammalian pets should be quarantined. If smallpox vaccines are
available in the country, vaccination of high-risk close contacts should be
considered after a risk-benefit assessment. For severe cases, treatment with a
registered antiviral can be considered, if available in the country.
ECDC actions :
ECDC will continue to
monitor this event through epidemic intelligence activities and report relevant
news on an ad-hoc basis. ECDC published a news item on 19 May, with initial
recommendations. An epidemiological update will be posted on 20 May. Multi-lateral
meetings between affected countries, WHO IHR and ECDC have taken place to share
information and coordinate response. A process in EpiPulse has been created to
allow countries to share information with one another, WHO, and ECDC. The
production of a Rapid Risk Assessment has been launched with prospective
publication on Monday 23 May.
Source:https://www.ecdc.europa.eu/en/news-events/epidemiological-update-monkeypox-outbreak
Biofilm Producing Pseudomonas aeruginosa in Patients with Lower Respiratory Tract Infections
Sabina Chhunju¹, Tulsi Nayaju1,
Kabita Bhandari1, Khadga Bikram Angbuhang1, Binod Lekhak3,
Krishna Govinda Prajapati², Upendra Thapa Shrestha3*, Milan Kumar Upreti1
¹GoldenGate International College,
Battisputali, Kathmandu, Nepal
²B&B Hospital. Gwarko, Lalitpur, Nepal
3Central Department of Microbiology, Tribhuvan University, Kirtipur, Kathmandu,
Nepal
*Corresponding author: Upendra
Thaha Shrestha, Central Department
of Microbiology, Tribhuvan University, Kirtipur, Kathmandu, Nepal; Email:
upendrats@gmail.com
ABSTRACT
Objectives: To
determine the prevalence of Gram-negative bacteria in lower respiratory tract
infections and study the biofilm producing Pseudomonas aeruginosa.
Methods: This study was
conducted at B & B Hospital Pvt. Ltd., Lalitpur, Nepal from February to
September 2018. The samples were collected from the patients (n=420) with signs
and symptoms suggestive of LRTIs. The isolated organisms were identified and
antimicrobial sensitivity was performed. Among all the isolates, P.
aeruginosa isolates were
subjected for biofilm detection by microtiter plate method.
Results: Out
of 420 specimens, 90 (21.6%) were culture positive. Klebsiella pneumoniae (42.9%)
was found to be the predominant organism with higher rate of resistance to
antibiotics. A total of 25 isolates of P. aeruginosa were isolated among
which 15 (60%) were biofilm producers. Biofilm-producing isolates of P.
aeruginosa were found more resistant to the tested antibiotics.
Conclusion:
Gram-negative bacteria were found to be the predominant etiological agents in
causing the LRTIs; K. pneumoniae, being
the most commonly isolated bacteria. Most P.
aeruginosa were capable of producing the biofilm. The biofilm producers
were more resistant to the antibiotics. The biofilm may help increase the
resistivity nature of the bacteria.
Keywords: LRTI, Gram-negative bacteria, Biofilm, Antibiotic resistance, MDR

Microbial quality analysis of panipuri samples collected from different parts of Bhaktapur
Punam Ghimire1, Sujata Khand1, Bhawana Chaulagain1, Ashish Siwakoti1, Dinesh Dhakal1, Upendra Thapa Shrestha2 *
1Sainik Awasiya Mahavidhyalaya
(affiliated to Tribhuvan University) Sallaghari, Bhaktapur
2Central Department of Microbiology,
Tribhuvan University, Kirtipur, Kathmandu, Nepal
*Corresponding Author: Upendra Thapa
Shrestha, Central Department of Microbiology, Tribhuvan University, Kirtipur,
Kathmandu, Email: upendra.thapashrestha@cdmi.tu.edu.np /
upendrats@gmail.com
ABSTRACT
Objectives: The study was aimed to identify
potential bacterial pathogens from the panipuri samples collected from
different vendors of Bhaktapur district and determine their antibiogram
patterns.
Methods: Altogether 120 (40 puri, 40 stuffing
and 40 pani) samples of panipuri were collected from different vendors of
Bhaktapur district in a cold chain and were transported to the microbiology
laboratory. Puri and stuffing were then pre-enriched, enriched and cultured
while pani samples were processed using the MPN method. All the isolates were
identified following standard microbiological procedure and subjected to
antibiotic susceptibility testing following CLSI guidelines.
Results: The result revealed contamination
of 77.5% stuffing, 67.5% puri and 52.5% pani samples with pathogenic bacteria. Among
bacterial pathogens, the highest number was Staphylococcus aureus
followed by Escherichia coli and Salmonella spp. 100% of S.
aureus were found to be resistant to ampicillin and novobiocin. Similarly,
94.1% of E. coli were resistant to ampicillin followed by ciprofloxacin
(64.7%). A very few isolates of Salmonella spp, Shigella spp and Vibrio
spp were resistant to tetracycline. The highest number of multidrug-resistant
bacteria were S. aureus, followed by Klebsiella
spp and E. coli.
Conclusion: The study showed that the panipuri
samples from street vendors were found to be highly contaminated with
pathogenic bacteria which might affect consumers’ health. Thus, to prevent any
food-borne illness in the future, frequent evaluation and regulation of the
quality of such foods should be carried out.